About PBC
PBC is an autoimmune liver condition. This page details what PBC is, how it is diagnosed, and how the disease and its symptoms can be monitored.
- PBC IS AN AUTOIMMUNE DISEASE THAT AFFECTS THE LIVER.
- IT IS CLASSED AS A COMMON RARE DISEASE.
- PBC AFFECTS NINE WOMEN TO EVERY ONE MAN.
- THE COMMON AGE OF DIAGNOSIS IS BETWEEN 35 & 55.
- THERE ARE WITH AN ESTIMATED 22,000 PBC PATIENTS IN THE UK.
- PBC IS BECOMING MORE COMMONLY DIAGNOSED.
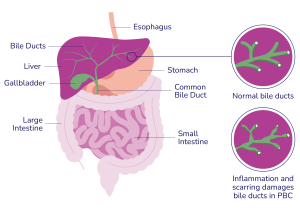
These bile ducts are designed to allow the flow of bile from the liver, so damage of these ducts leads to poor drainage of bile acids. The bile acids then leak from the bile ducts, damaging surrounding liver cells, which then causes inflammation and scarring in the liver.
This widespread damage and scarring may result in cirrhosis, however most people with PBC will never develop cirrhosis. Cirrhosis is often assumed to mean damage to the liver caused by excessive alcohol consumption. But this is not the case: cirrhosis simply means an advanced form of scarring, which changes the structure of the liver cells. Cirrhosis can be caused by many liver and biliary diseases. Whatever the cause, cirrhosis can lead to a number of potential problems requiring long-term monitoring by your clinician.
PBC was formerly known as Primary Biliary Cirrhosis. In 2015, the name was changed to Primary Biliary Cholangitis. The word “Cholangitis” refers to inflammation of the cholangiocytes (bile duct cells). This means that for the vast majority of people with PBC, the name is far more accurate, with less of the negative experiences associated with the word cirrhosis.
We understand more and more about PBC each year. Whilst we know that two aspects need to be in place for someone to develop PBC: a genetic element (predisposition) and an environmental trigger, we do not know what causes PBC or what can cure PBC.
There are however treatments that can help people with PBC to manage their disease progression and symptoms. Ursodeoxycholic Acid (also called Urso or UDCA) is the first-line treatment for PBC, it is a bile salt which enables bile to be drained from the liver, slowing down the progress of the condition in terms of cell change, and often results in lower Liver Function Tests (LFTs). Patients with PBC who respond to Urso, known as Urso-responders are thought to rejoin the general populace in terms of life expectancy.
Approximately 20-30% of patients do not respond effectively to Urso. These patients will need to be monitored closely and continue a more detailed partnership with their clinician. In 2017, a secondary therapy, Obeticholic Acid (OCA) was approved, and we are excited that new treatments are currently being developed and assessed.
We are often asked about PBC and familial links. Due to the genetic predisposition, there is a slightly increased risk of your first-degree relatives (especially mother/daughter) having PBC. However, that risk is still very small. You cannot pass on PBC by normal contact, by blood, sex, or breast feeding, and at present we do not recommend routine testing of relatives who are well.
There is much false information, and many out-of-date studies still available on the internet that don’t paint the brightest picture for PBC patients. But the current reality is that most patients will die with their PBC and not because of their PBC. In fact, our oldest member of the PBC Foundation community was 103 when she died ‘with’ her PBC, not ‘from’ it. More and more patients are now speaking of being diagnosed 20+, 30+ years and that will continue to grow as improvements in treatment (even historically) lead to better and longer survival.
Diagnosis
As awareness of the condition improves, along with technology, many patients are being diagnosed younger or earlier in their disease journey than previously experienced. Diagnosis of PBC is made on the presence of at least two of the three following features:
Monitoring PBC
One of the key aspects of living with PBC is lifelong surveillance, including monitoring of symptoms, or of liver biochemistry, and taking into account Urso-response and the most appropriate care pathway for each patient.
When it comes to managing your PBC, you can make a real difference. Whilst your doctor keeps track of several aspects to help monitor your condition. Understanding what these are and how they affect you, allows you to become better informed and connected with your PBC.
The following three aspects of PBC, all need to be monitored, and addressed, separately:




Please bear in mind that the information on this website does not replace the value of a personalised conversation with a trained member of staff with a good working knowledge of PBC, so if you do have any questions, please contact a medical expert. If you are inspired to read more about PBC, our Compendium is available to all registered service users. It has been designed to be your PBC companion, your friend, your reference guide. Please visit our reference library to download any of our leaflets and publications.

